Nebulization therapy for mechanically ventilated patients
Mechanical ventilation is required in 50% to 70% of critically ill patients, and nebulization is one of the intensive airway management methods often used in conjunction with mechanical ventilation.
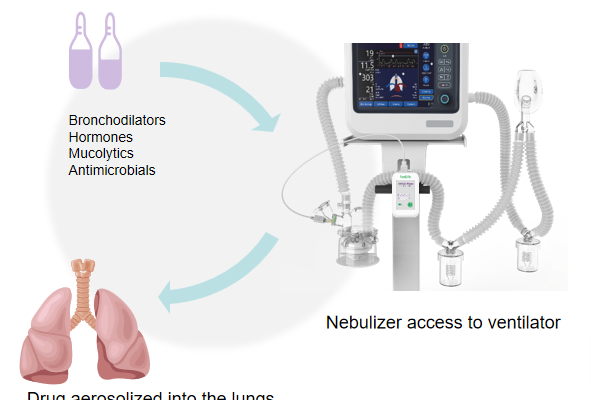
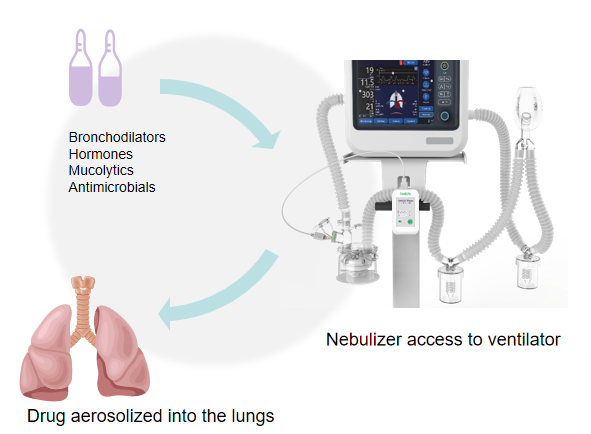
Nebulization (aerosol inhalation therapy) is the bronchodilators, hormones or antimicrobial drugs made into an aerosol, in the form of an aerosol or mist transported into the airways and lungs, so as to achieve the purpose of treatment of disease or symptomatic relief of the Mechanical ventilation nebulization therapy, the aerosol from the nebulizing device produced transported into the respiratory line, and transported to reach the lower respiratory tract under the effect of positive pressure.
Nebulization is different from wetting:
Wetting refers to a physical therapy that applies a humidifier to disperse water into water vapor under a certain temperature control and sprays it into the respiratory tract at a certain speed to moisten the airway mucosa, dilute sputum, and maintain the normal movement and contouring function of the respiratory mucus cilia system.
Timing of nebulization administration in patients with noninvasive ventilation
Compared with nebulization during the interval of noninvasive ventilation, nebulization during noninvasive ventilation:
- shortened duration of mechanical ventilation
- greater comfort for patients with COPD respiratory failure
- Lower incidence of adverse events
- probability of pharyngeal discomfort may be lower
Noninvasive ventilation combined with nebulized inhalation can effectively improve clinical symptoms in patients with acute exacerbation of COPD (AECOPD). Two different modes of nebulized inhalation may be used when applying sputum chemotherapeutic agents, bronchodilators, and hormonal nebulized therapy in patients with noninvasive ventilation.
The systematic evaluation included 12 RCTs comparing nebulization during noninvasive ventilation with nebulization between noninvasive ventilation intervals, of which 5 RCTs reported relevant clinical outcomes: mean length of hospital stay, duration of mechanical ventilation, adverse effects, and patient comfort, while the other studies did not report clinical outcomes for the patients, and 1 other study is ongoing.
Why Choose The Air ICU Series?
Experiments have demonstrated that the mesh nebulizer is currently the most ideal nebulizing device for delivering inhaled preparations for use in conjunction with a ventilator.
Compared to compression nebulizers, mesh nebulizers have a higher delivery efficiency than compression nebulizers when used in conjunction with a ventilator [1].
Compared to ultrasonic nebulizers, ultrasonic nebulizers have been used less frequently in clinical practice due to the inability to nebulize viscous solutions, the potential for the heat generated to destroy the solution, and larger residues [2].
Compared to pMDI and due to difficulty in synchronizing inhalation, pMDI reduces drug delivery and drug dose may change due to separation from the ejection agent [3].
Air ICU is a new generation of professional mesh nebulizer with feellife core patents.
It is embedded with AiMesh®inside polymer diaphragm technology and breath sensing technology.
[1] Berlinski A and Willis JR. Albuterol delivery by 4 different nebulizers placed in 4 different positionsin a pediatric ventilator in vitro model. Respiratory care.2013,58:1124-33.
[2] Ari A and Fink JB. Guidelines for aerosol devices in infants, children and adults: which to choose, why and how to achieve effective aerosol therapy. Expert review of respiratory medicine.2011;5:561-72.
[3] Diot P, Morra Land Smaldone GC. Albuterol delivery in a model of mechanical ventilation. Comparison of metered-dose inhaler and nebulizer efficiency. American journal of respiratory and critical care medicine.1995;152:1391-4.